

Is 2 Weeks Enough To Test Clean


 Besides run across: Overview of Oral Fluid Testing
Besides run across: Overview of Oral Fluid Testing
California NORML Guide
Interpreting Drug Examination Results
Contents:
Drug Test Detection Times: summary for dissimilar drugs and detection technologies.
Detection Time for Marijuana in Urine: Urine tests detect non-psychoactive marijuana metabolites for days to weeks after use, long after impairment has passed.
Detection Fourth dimension for Marijuana in Blood : Blood tests can detect presence of active THC; high levels indicate recent employ, low levels may persist for hours or days.
Marijuana Use and Accident Risks : Accident studies show no relation between urine test results and accident run a risk; presence of THC in blood a moderate gamble factor, comparable to low levels of blood alcohol below threshold of DUI; high levels of THC or combination of THC with alcohol indicative of DUI.
Drug Test Detection Times for Marijuana
How long practice drug tests detect marijuana? There is no uncomplicated answer to this question. Detection time depends strongly on the kind and sensitivity of the test employed; the frequency, dosage, and last time of utilise; the private subject area's genetic makeup, the state of i's metabolism, digestive and excretory systems; and other random, unknown factors.
The bones drug test types and their approximate detection times are shown in the tabular array below.
| Urine | Claret | Pilus | Saliva | |
| Marijuana – Unmarried Use | 1-7+ days | 12-24 hrs | Hundred-to-one | Not validated (0 -24 hours?) |
| Marijuana – Regular Use | 7-100 days | 2-vii days | Months | |
| Amphetamines | ane-3 days | 24 hours | ||
| Cocaine | 1-3 days | 1-iii days | ||
| Heroin, Opiates | 1-4 days | i-three days | ||
| PCP | 3-7 days | i-3 days |
The about popular kind of drug test is the urine examination, which can detect marijuana for days or weeks after use. Note that urine tests do not detect the psychoactive component in marijuana, THC (delta-9-tetrahydrocannabinol), and therefore in no mode measure impairment; rather, they detect the non-psychoactive marijuana metabolite THC-COOH, which can linger in the torso for days and weeks with no impairing effects. Because of THC-COOH's unusually long elimination time, urine tests are more than sensitive to marijuana than other commonly used drugs. According to a survey by Quest Diagnostics, 50% of all drug test positives are for marijuana.
Claret tests are a better detector of recent use, since they measure the active presence of THC in the arrangement. Because they are invasive and difficult to administrate, blood tests are used less frequently. They are typically used in investigations of accidents, injuries and DUIs, where they can give a useful indication of whether the subject was actually under the influence.
Pilus tests are the nearly objectionable form of drug testing, since they do non measure electric current apply, but rather non-psychoactive residues that remain in the hair for months later. These residues are absorbed internally and do non appear in the pilus until 7-10 days after first utilise. Later on, they cannot be washed out past shampoos (though shampoos may aid remove external fume particles that get stuck in the pilus). Hair tests are more likely to notice regular than occasional marijuana use. One study found that 85% of daily users tested positive for marijuana, versus 52% of occasional smokers (1-5 times per calendar week). Ingested cannabis was less likely to be detected than smoked marijuana [01]. It is doubtful whether pilus tests are sensitive to one-time use of marijuana.
Saliva testing is a newer, less proven technology. The sensitivity of saliva tests is not well established in the case of marijuana. In theory, they are supposed to detect contempo use, only this may range from several hours to over a day. They are supposed to detect secretions from inside the oral tissues that cannot be washed out with mouthwash. Because they are less intrusive than blood or urine tests, the industry has been eager to develop saliva tests. Due to reliability problems, they have yet to gain credence in the U.S., just they have come into use in some other countries, such as Australia. An international report of various onsite saliva tests concluded that no device was reliable enough to exist recommended for roadside screening of drivers (Rosita Project, 2003-2006).
Urine Testing Detection Times for Marijuana
How long marijuana is detected in the urine depends strongly on frequency of use. In regular users (more than than one time a week), the marijuana metabolite THC-COOH builds up to a high level, often on the order of hundreds of nanograms per milliliter (ng/ml), from which it may take weeks to decline back below the threshold of detection. The state of affairs is unlike for occasional users (no more than once a week), who often clear up in a couple of days.
Figure 1 illustrates typical urine testing profiles for "i-fourth dimension" users – that is, subjects who were clean before going into the test. This would typically be the instance for the occasional user who indulges a couple of times per month.
(Data on Subjects B, G, Due east from Huestis and Oral bailiwick from Constabulary).
Subjects B and G illustrate typical "ane-fourth dimension" responses in a group of study subjects. All subjects received a dose of one standard NIDA cigarette [02]. They were monitored for urine levels of marijuana metabolite (THC-COOH) at regular intervals after smoking. Both B and 1000 were positive at the standard cutoff threshold of l ng/ml (the standard in most government-required testing programs) for up to two days afterwards smoking.
Note that urine levels of metabolite fluctuate throughout the twenty-four hour period. For case, Bailiwick G fell beneath the fifty ng threshold around 24 hours subsequently smoking, but rebounded to a higher place it a short time afterward. Thus it is possible to flunk a drug test despite having passed 1 a while earlier.
Subject field "Eastward" was an infrequent subject who never exceeded l ng/ml despite having smoked the same dose as other report subjects. This illustrates the high degree of private variation in urine testing. While Subjects G and B would likely have flunked a drug examination the twenty-four hour period after smoking, Subject area E wouldn't have.
Occasional use can sometimes be detected much longer, equally shown in Fig. 1 by the oral dose from a different controlled study [03]. This represents a subject who was given a strong oral dose of xx mg of THC, equivalent to a potent credibility or 2 high-dose Marinol pills. The subject tested above the 50 ng/ml cutoff for up to six days later dosing. California NORML has heard unconfirmed reports of occasional users testing positive for as long as two weeks in infrequent cases. In most cases, however, 1-time users are likely to pass after a couple of days.
Fourth dimension to kickoff positive exam
Drug metabolites take time to achieve the urine. A user who is make clean beforehand tin exam negative for over i – 4 hours before turning positive at 50 ng/ml, equally shown in the following data from Huestis [02]. This is similar to the period of impairment after smoking. Therefore, in the instance of i-fourth dimension users, a positive urine test is a sign that the user is well-nigh likely NOT currently dumb by marijuana!
Figure 2 – Drug Testing Profiles in Offset Hours Following Single Use
(Early Urine Examination Profiles from Huestis et al. [2])
Urine Testing in Regular Users
In regular users, metabolite levels can build up to background levels in a higher place one,000 ng/ml. Many days or weeks of forbearance are required to articulate out, as illustrated in the following graph of metabolite levels in examination subjects who were regular users [04A].
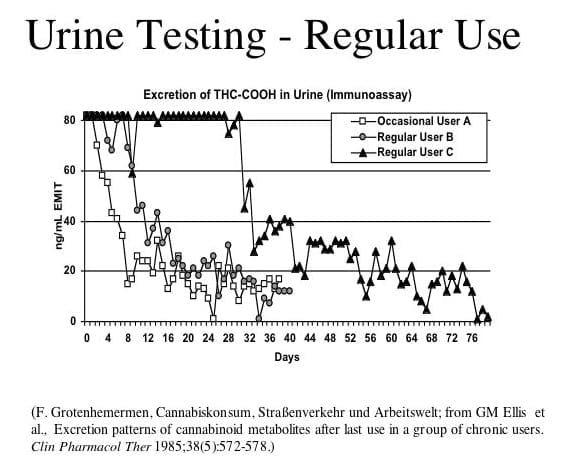 Subject B took over a calendar week to fall below the l ng/ml cutoff, while Subject C took a calendar month. Detection times over 3 months accept been reported in farthermost cases.
Subject B took over a calendar week to fall below the l ng/ml cutoff, while Subject C took a calendar month. Detection times over 3 months accept been reported in farthermost cases.
Note that it is possible to test negative on one mean solar day, then positive on the next.
Equally shown in the post-obit graph, detection times for chronic users typically range from one to three weeks merely tin can extend much longer. In this study by Ellis [04], chronic users were tested at xx ng/ml and 100 ng/ml, but not at the normal standard of l ng/ml.
Blood Tests
Unlike urine tests, blood tests discover the active presence of THC in the bloodstream. In the case of smoked marijuana, THC peaks rapidly in the beginning few minutes later on inhaling, oftentimes to levels above 100 ng/ml in blood plasma. It then declines rapidly to single-digit levels within an 60 minutes. High THC levels are therefore a good indication that the subject has smoked marijuana recently. THC can remain at low but detectable levels of 1-ii ng/ml for eight hours or more than without any measurable signs of harm in ane-time users. In chronic users, detectable amounts of blood THC can persist for days. In one study of chronic users, residue THC was detected for 24 to 48 hours or longer at levels of 0.5 – 3.two ng/ml in whole blood (1.0 – half-dozen.4 ng/ml in serum) [Skopp and Potsch].
Annotation: THC blood levels can be measured in two ways. Almost labs used past U.S. law enforcement report levels based on concentration in whole blood, but others written report concentration in blood serum or plasma instead. Concentrations in whole claret are about half every bit high equally those in serum/plasma. Therefore 0.5 – 3.two ng/ml in whole blood = ane.0 – 6.4 ng/ml in plasma or serum. Unless otherwise stated, whole blood concentrations are reported hither.
In another report of 25 frequent users, 36% showed no measurable blood THC throughout 7 days of abstinence, while the rest had at least one positive, though not necessarily on the first day. Vi subjects (24%) had detectable blood THC after seven days at levels ranging from 0.2 to i.v ng/ml (that is, 0.4 to three.0 ng/ml in serum) [Karschner]. There have been anecdotal reports of even higher solar day-afterwards blood THC levels in chronic users, but these oasis't been confirmed in controlled studies.
Dissimilar urine, blood test results can requite a useful indicator of whether 1 is under the influence of marijuana. Studies have shown that high THC blood levels are correlated with impaired driving. An expert panel review of scientific studies on driving under the influence of cannabis concluded that THC levels above 3.5 – v ng/ml in claret (or 7 – 10 ng/ml in serum) indicate probable damage [Grotenhermen]. The same review found no increased driving hazard at low levels of THC. Despite the fact that accident studies have repeatedly failed to find evidence of increased driving chance at low levels (one or 2 ng in claret) of THC, numerous states and strange countries have enacted "nada-tolerance" laws, treating any non-cypher trace of THC equally legal evidence for driving under the influence. Others have stock-still, per se limits above which DUI is presumed, oftentimes with no scientific basis. However, nigh states (including California) don't have per se limits, but define DUI in terms of whether the totality of bear witness (including drug exam results) shows that the driver was impaired by marijuana or drugs.
Although high claret THC is a fairly skillful indicator of beingness under the influence, information technology is non infallible. Chronic users who develop tolerance to THC may in some cases drive safely with very high blood levels of THC. In one study, a subject with severe attention deficit disorder could not pass a driving examination while straight, but performed well with a blood level of 71 ng/ml [Strohbeck-Grandühner]. No similar miracle is known for alcohol.
Oral ingestion
Oral ingestion produces a much different THC blood profile than smoking. Instead of peaking sharply, THC rises gradually over a couple of hours to a plateau of around ii.v – 5 ng/ml in claret (5 – 10 ng/ml in serum), then declines (run across blue curve in Figure 5).
Claret metabolites
In improver to THC, blood tests can find cannabinoid metabolites. Non exceptionally, labs study levels of THC-COOH, the same not-psychoactive metabolite found in urine. As shown in Fig. 5, THC-COOH levels for claret are similar to urine. They may be detectable for a couple of days after a single use or weeks in chronic users, and are therefore not a valid indicator of being nether the influence. There is no scientific ground for treating drivers who have THC-COOH but non THC in their blood every bit being legally "under the influence."
Another claret metabolite non shown in Figure 5 is xi-hydroxy-THC, a psychoactive byproduct produced when THC is processed by the liver afterwards oral ingestion. While not detectable at observable levels in smoked marijuana, 11-hydroxy-THC shows a similar claret profile to THC afterward oral consumption. The presence of 11-hydroxy-THC may therefore exist used as an indicator of recent oral utilize. However, about blood tests don't carp to cheque for 11-hydroxy-THC.
Effigy 5 – Blood plasma levels of THC & Metabolite
References:
(A-B) Smoked dose based on information from G. Huestis , J. Henningfield and E. Cone,K. Huestis , J. Henningfield and E. Cone.
(C) Oral dose based on information from B. Law et al.
Drug Exam Results and Accident Adventure
Drug tests are oft used indiscriminately as an indicator of driving under the influence of cannabis (DUIC). As nosotros take seen, in that location is no scientific basis for using urine tests to determine whether one is really dumb by marijuana, since they only measure the non-psychoactive metabolite THC-COOH. Unfortunately, this has non prevented ignorant lawmakers in certain states from passing "zero-tolerance" laws that define the presence of any cannabis metabolites to be proof of DUIC.
The situation is somewhat more complicated with respect to claret tests for THC, since high levels of THC may exist correlated with impairment, though depression levels less than three-5 ng/ml are not. In one case again, this has not deterred many lawmakers from passing "zero-tolerance" laws for THC, even though DUI laws typically allow low blood levels of alcohol.
Fortunately, most states (like California) do not accept a zilch-tolerance DUI standard for drugs, but rather require the prosecutor to testify that the driver'southward operation is really drug-dumb in order to get a DUIC conviction. In this event, the driver'due south guilt is determined past the totality of evidence in the case: driving behavior, performance on roadside sobriety tests, the driver's deport, the aroma of smoke in the machine – and also drug test results. Defendants can then win amortization if they can convince the court they were not dumb, regardless of drug test results.
Accident Studies
Numerous accident studies have confirmed that marijuana is not a major risk gene in driving fatalities. A recent meta-assay of 42 different studies on cannabis and driving ended that the odds of a fatal blow due to cannabis use are only 1.25 times normal, significantly less than many other risks such every bit historic period, gender, and alcohol use [Elvik]. The written report found higher fatal accident odds for opiates (one.44), benzodiazepine tranquilizers (2.thirty), anti-depressants (one.32), cocaine (2.96), amphetamines (iv.46) and the sleeping help zopiclone (two.threescore). Booze wasn't included, but has elsewhere been calculated at 2 to 6, depending on claret level.
Table 2 summarizes studies that take assessed the accident risk for drivers with traces of marijuana in their system. The studies surveyed fatal accidents, looking at levels of marijuana, alcohol and other drugs in the commuter's blood or urine.
For each blow, researchers make up one's mind the degree to which the driver was responsible for the blow. Using this data, they compute a "culpability ratio," comparing the adventure of accidents for drug-positive drivers to drug-costless drivers. A culpability ratio of 1 ways no increased risk; above 1 hateful increased adventure; and beneath 1 means reduced risk. Culpability factors above 3 or iv are considered notably significant.
Equally shown in the quaternary column of Tabular array 2, drivers with high claret alcohol levels (above the standard legal limits of .08% or .10%) showed consistenly high culpability ratios, on the guild of five or half dozen. In dissimilarity, drivers with THC present in their blood rarely exceeded 2, and in several cases were less than 1 – indicating they were actually safer than drug gratis drivers! This phenomenon has been explained by the fact that marijuana-using drivers tend to deadening down, while alcohol-using drivers tend to speed.
I exception is the 2004 study by Drummer et al, which did not count drivers with less than i nanogram THC in blood. The remaining THC-using drivers had an average culpability ratio of 2.7, which is similar to the risk ratio for drivers with moderate amounts of alcohol in their arrangement (as shown in the studies by Laumon and Bédard, which looked at drivers with blood booze content less than 0.05%, a legal amount in the U.S.).
Note that the Drummer report establish especially loftier culpability for drivers with five or more nanograms blood THC, comparable to the adventure for drunken drivers. This confirms that loftier blood THC, indicating recent usage, is a sign of probable harm, while lower levels, which remain for several hours, are not.
Table ii does not include culpability data for drivers with both alcohol and THC in their arrangement (that is, all of the marijuana drivers were alcohol-gratuitous). In general, studies concord that the combination of alcohol and THC is particularly dangerous, if anything worse than "straight" drunken driving.
Not surprisingly, no elevated risk was institute in the 3 studies listed at bottom, which looked at urine metabolite levels rather than blood THC. This confirms that urine testing has no bearing on driving damage. Despite this fact, US Department of Transportation regulations force millions of commercial drivers to submit to random urine testing. The government has never produced convincing scientific evidence that this policy is necessary or effective to protect public safety. But they're the government, so they don't have to provide whatsoever show!
Table two – DUI Blow Culpability Studies
| Location | # Drivers | Study | Culpability Ratio Claret booze content=.08-.10% | Culpability Ratio THC (just) |
| New York | 497 | Terhune & Cruel (1982) | 5.7 | 2.i |
| California | 440 | Williams et al. (1985) | 5.0 | 0.2 |
| U.Due south. | 1,882 | Terhune et al. (1992) | 5.7 | 0.7 |
| Australia | 1,045 | Drummer (1994) | five.5 | 0.7 |
| Australia | 2,500 | Longo and Hunter (2000 & 1998) | 6.8 | 0.9 0.36(<ane ng/ml) 1.8 (>2 ng/ml)* |
| Australia | 2,298 | Drummer et al (2004) | 6.0 | two.7 (>1 ng/ml) 6.vi(>5 ng/ml)* |
| France | x,748 | Laumon (2005) | 3.0 – 6.2 (BAC=.10) 2.01 (BAC=.05) | 1.78 |
| U.South. | 32,543 | Bédard (2007) | 8.51 (3.3 BAC =.05) | 1.29 |
| Studies Looking at Urine Metabolites of Marijuana | ||||
| Netherlands | 110 cases + 816 controls | Movig (2003) | 5.46 (BAC .05–.08) xv.five BAC >.08 | 1.22 (urine and/or claret) |
| Colorado | 414 | Lowenstein et al (2004) | 3.2 | 1.1 (urine) |
| Maryland | 5,573 | Soderstrom et al (2005) | 7.45 | i.two (urine) |
* THC concentration measured in whole claret
Summary: Interpreting Drug Tests in Lite of DUID Accident Studies
- THC-COOH metabolite in urine (or blood) Non correlated to accident gamble!
- Presence of THC (just) in blood: LESS OR EQUAL TO RISK of booze at .05% (below legal DUI threshold)
- Claret THC = v ng: risk COMPARABLE to DUI
- Blood THC = ii ng = NO increased risk
- THC + alcohol = HIGH DUI risk
- Stimulants (cocaine, amphetamine, etc) = MODERATE adventure (~alcohol at .05%)
Footnotes
[01] M Huestis et al., "Cannabinoid concentrations in pilus from documented cannabis users," Forensic Scientific discipline International (Aug 2006). Available at world wide web.sciencedirect.com.
[02]Thousand Huestis, J Mitchell and Eastward Cone, "Urinary Excretion Profiles of 11-Nor-ix-Carboxy-Delta-ix-Tetrahydrocannabinol in Humans later Unmarried Smoked Doses of Marijuana," Journal of Analytical Toxicology, Vol twenty:441-52 (Oct 1996).
[03] B. Police et al, "Forensic aspects of the metabolism and excretion of cannabinoids following oral ingestion of cannabis resin," J. Pharm. Pharmacol. 36: 289-94 (1984).
[04A] Courtesy of F. Grotenhermen, adopted from K Ellis et al, "Excretion patterns of cannbinoid metabolites after last use in a group of chronic users," Clin. Pharmacol. Ther. 38:572-eight (1985).
[04] G Ellis et al, "Excretion patterns of cannbinoid metabolites after concluding use in a group of chronic users," Clin. Pharmacol. Ther. 38:572-8 (1985).
[05] F Grotenhermen et al., "Developing limits for Driving under cannabis, Habit Vol. 102#12: 1910-7 (Dec 2007). As well, "Developing Science-Based Per Se Limits for Driving Under the Influence of Cannabis: Findings and Recommendations by an Expert Panel" https://www.canorml.org/healthfacts/DUICreport.2005.pdf.
[06] Strohbeck-Kühner et al, "Fahrtüchtigkeit trotz (wegen) THC" ["Driving power despite (or because of) THC"], Archiv für Kriminologie 220:11-xix (2007).
[06a] G Skopp and L Potsch, "Cannabinoid concentrations in spot serum samples 24-48 hours afterwards discontinuation of cannabis smoking," Journal of Belittling Toxicology 32: 160-4 (2008).
[07] EL Karschner et al. "Practice Delta(9) THC concentrations betoken recent employ in chronic cannabis users?," Habit, Oct. 5, 2009 http://www.ncbi.nlm.nih.gov/pubmed/19804462.
[08] M. Huestis , J. Henningfield and Due east. Cone,"Blood Cannabinoids. I. Assimilation of THC and Germination of xi-OH-THC and THCCOOH During and After Smoking Marijuana”,Journal of Analytic Toxicology, Vol. 16: 276-282 (1992).
[09] Elvik, R. , "Risk of road accident associated with use of drugs: A systematic review and meta-analysis of show from epidemiological studies," Accident Analysis and Prevention (July 26, 2012).
Tabular array two Accident Studies:
Terhune, Thousand.W. & Fell, J.C. The Role of Booze, Marijuana, and Other Drugs in Accidents of Injured Drivers. Technical report for the National Highway Traffic Safety Assistants, U.Due south. Dept of Transportation, NTIS Report No. DOT-HS-806-181. Springfield, VA (1982).
Williams, A.F. et al. Drugs in fatally injured immature male drivers. Public Health Reports 100: 19-25 (1985).
Terhune, K.W. et al. The incidence and office of drugs in fatally injured drivers. Washington: United states Dept. of Transportation, National Highway Traffic Safety Administration; Study No. DOT-HS-808-065 (1992).
Drummer, O.H. Drugs in drivers killed in Australian road traffic accidents. Victorian Institute of Forensic Pathology, Establish of Forensic Medicine, Monash Academy, Melbourne, Australia, Report No. 0594 (1994).
Longo, 1000.C. et al. The prevalence of booze, cannabinoids, benzodiazepines and stimulants amongst injured drivers and their role in driver culpability: Part ii: the human relationship between drug prevalence and drugculpability. Accid. Anal. Prev. 32, 623–32 (2000).
C. Hunter, R. Lokan, M. Longo, J. White, 1000. White, The prevalence and role of alcohol, cannabinoids, benzodiazepines and stimulants in non-fatal crashes, Department for Administrative and Information Services, Adelaide, Due south Australia, 1998.
Drummer, O.H. et al.The interest of drugs in drivers of motor vehicles killed in Australian road traffic crashes. Accid. Anal. Prev. 36, 239–48 (2004).
Laumon, B. et al. Cannabis intoxication and fatal route crashes in French republic: population based case-control study. British Medical Periodical, 331:1371 doi:ten.1136/bmj.38648.617986.1F (Dec 10, 2005).
Bédard, One thousand, Dubois, Southward, and Weaver, B. The impact of cannabis on driving. Canadian Journal of Public Health, 98#one:6-xi. (Jan-February 2007).
Movig, KLL et al. Psychoactive substance use and the risk of motor vehicle accidents. Accident Analysis and Prevention 36: 631-6 (2004).
Lowenstein, S and Koziol-McClain, J. Drugs and traffic crash responsibility: a written report of injured motorists in Colorado. Journal of Trauma, Injury, Infection, and Disquisitional Care l#2: 313-20 (2001).
Soderstrom, C et al. Crash Culpability Relative to Age and Sex for Injured Drivers Using Alcohol, Marijuana, or Cocaine. 49th Almanac Proceedings, Clan for the Advancement of Automotive Medicine, pp.320-41 (Sep 12-14, 2005).
Besides see: California NORML's Drug Testing Tips – Dealing With Urinalysis on Curt Notice

Source: https://www.canorml.org/employment/marijuana-drug-test-detection-times/
Posted by: shrumofflas.blogspot.com
0 Response to "Is 2 Weeks Enough To Test Clean"
Post a Comment